Can Delivery Room CPAP Reduce the Rate of BPD in Preterm Infants?
- Published on:
Can Delivery Room CPAP Reduce the Rate of BPD in Preterm Infants?
- Published on:

On this page
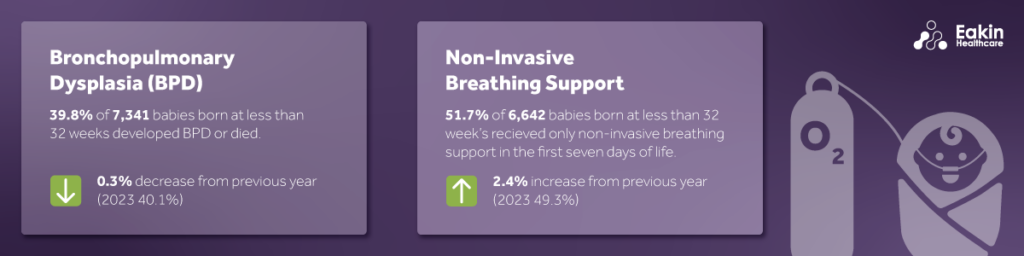
Bronchopulmonary dysplasia (BPD) is defined as the requirement of respiratory support at 36 weeks post menstrual age in an infant born before 32 weeks. BPD is a common complication seen in preterm babies, nationally 39.8% of babies born before 32 weeks’ gestation developed BPD or died according to National Neonatal Audit Programme (NNAP) data for 2024.[1] Rates of BPD in preterm babies have remained constant over recent years.
Why Early Respiratory Support Matters
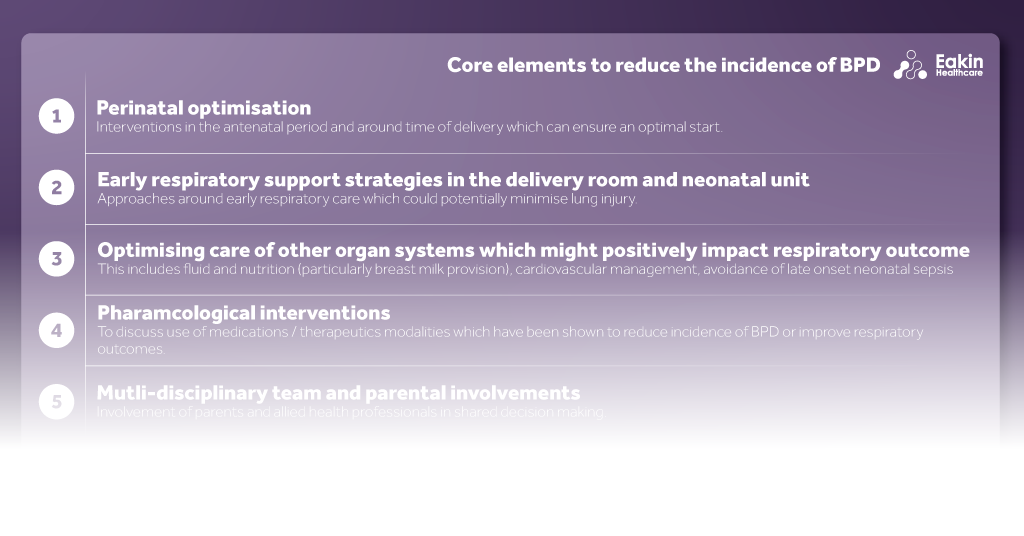
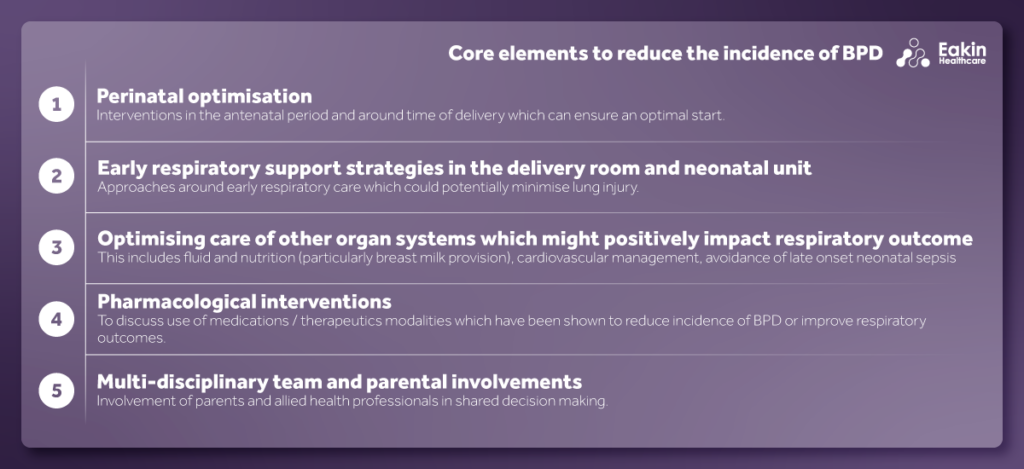
Premature babies have immature lungs and often require breathing support soon after birth. Ventilation of preterm babies is associated with barotrauma, inflammation and lung injury. Invasive ventilation commenced within 24 hours of birth is recognised as a risk factor for developing BPD.[2] Providing non-invasive respiratory support and avoiding mechanical ventilation is recommended as a strategy to reduce the risk of BPD. Supporting transition of preterm babies with a gentle approach is key. For stabilising preterm babies at delivery, NICE guidance recommends the use of continuous positive airways pressure (CPAP), rather than invasive ventilation.[2] The European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update, also recommends that for spontaneously breathing preterm infants, CPAP initiation rather than intubation will reduce lung injury and BPD.[3] More recently, the BAPM toolkit on the topic of BPD identifies five core strategies to reduce the incidence of BPD.[4] Early respiratory support strategies in the delivery room and neonatal unit are one of these elements. A Cochrane review on the topic reported that prophylactic or very early CPAP, when compared to mechanical ventilation probably reduces the incidence of BPD, and death or BPD.[5] Expert consensus is to start with CPAP pressure at least 6 cm H2O[3] for example BAPM recommends using pressure between 6-8cm H2O.[4] Intubation should be reserved for babies who are not responding to intermittent positive pressure ventilation, such as babies who remain apnoeic or are unstable. Intubation can also be considered for the most extreme preterm babies, for example those born at 22-24 weeks[3] or those <24[4] although evidence is lacking and recommendations are based on expert consensus. Early surfactant, by less invasive surfactant administration (LISA) is recommended alongside early CPAP, usually offered as a rescue modality.[4]
Why CPAP Alone Is Not The Full Answer
However, NNAP report of data from 2023 showed that there was only a weak correlation between different units’ use of non-invasive breathing support in the first week and those units’ BPD rates.[6] They reported that, “units with higher rates of the composite outcome of BPD or death are, on average slightly less likely to have a high proportion of babies cared for using non-invasive breathing support alone.”[6] This likely reflects the multifactorial nature of BPD with interventions in the antenatal period and around the time of birth also recognised as core elements included in the BAPM toolkit to reduce the incidence of BPD. The toolkit helps us recognise the breadth of interventions to consider including those addressing other organ systems, the importance of nutrition in particular early maternal breast milk and the role of the multidisciplinary team in caring for infants at risk of BPD.[4]
National Trends In Non-Invasive Support
The use of non-invasive breathing support is increasing nationally. According to the last NNAP annual report, nationally 51.7% of babies born at less than 32 weeks received only non-invasive breathing support in the first seven days of life, an increase of 2.4% from the previous year.[1] However the NNAP report also notes there is significant variation in adherence to NICE guidance among neonatal units and networks, which is not decreasing over time.
Results in Bolton
Takeaway
BPD is multifactorial with early respiratory care being a key component. Delivery room CPAP is recommended by national and international guidelines alongside early LISA, and our experience is that it leads to improved outcomes in extremely preterm infants.

Dr Hannah Spierson
Consultant, Royal Bolton Hospital
Hannah completed her neonatal grid training in the Northwest in 2022 and has been working as a consultant in Bolton neonatal unit since. She has led various quality improvement projects relating to respiratory care of preterm babies in Bolton.