Does Faith in the Outcome Matter Most When Caring for Extremely Preterm Infants?
- Published on:
Does Faith in the Outcome Matter Most When Caring for Extremely Preterm Infants?
- Published on:
On this page
It is well known that outcomes for those born at 22-23 weeks gestation can vary greatly across neonatal units and countries. The central question though is how much of this variation is due to established biology and to what degree is outcome influenced by unit culture. Specifically, how much can units influence outcomes based on a willingness to intervene and belief that they can succeed?
Defining the Population — and the Challenge
Extremely preterm infants, defined as those born before 28 weeks’ gestation, represent one of the most fragile patient populations in medicine. Within this group, those born at 22–23 weeks remain at the threshold of viability, where survival is uncertain and morbidity is substantial.
These infants are at risk of significant complications including intraventricular hemorrhage, necrotizing enterocolitis, sepsis, patent ductus arteriosus, and chronic lung disease. Survival itself is not the only metric of course with neurodevelopmental impairment (NDI), cerebral palsy, and long-term sensory deficits in survivors coming into greater focus.
From Variation to Benchmarking: Who Are the “Best”?
Even among high-resource settings, outcomes for infants born at 22–23 weeks differ significantly across networks.
The work of the iNeo collaboration and others has made this difficult to ignore.[1] Some centres achieve survival rates that would have seemed implausible a decade ago.
A striking example comes from a single-center experience in Japan, where survival among infants born at 22 weeks reached 83%. A level for sure that challenges long-held assumptions.[2] These results force us to confront an uncomfortable question: are differences in outcomes due to patient factors, or differences in care philosophy?
As before, “faith”, defined as the belief that survival is possible and worth pursuing still appears to be a prerequisite for the task of caring for such vulnerable infants. Once your team has faith, the next step is to selectively choose which strategies to employ in the care for these tiny babies.
Redefining “Best Care”
Historically, “best care” was difficult to define. Today, we are moving toward a more measurable construct.
Recent Canadian Neonatal Network Follow-Up data highlight a critical shift. Outcomes are increasingly framed not just in terms of survival, but survival without major morbidity.[3]
The Central Battleground: Bronchopulmonary Dysplasia (BPD)
If there is a single complication that is central to modern extreme prematurity care, it is bronchopulmonary dysplasia (BPD).
BPD is not merely a respiratory diagnosis; its presence is associated with increased rates of neurodevelopmental impairment, prolonged hospitalization, and increased healthcare utilization.
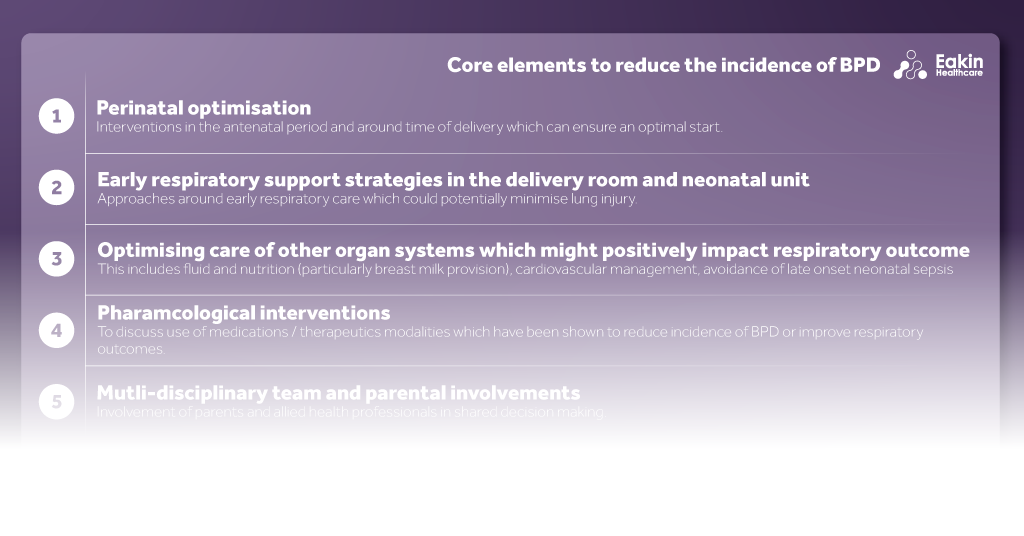
What is being explored to reduce rates of BPD?
1. Ventilation Strategies
The move toward lung-protective ventilation is now well established. Volume-targeted ventilation reduces ventilator-induced lung injury and has been associated with lower rates of severe IVH and periventricular leukomalacia.
High-frequency modalities including HFOV with volume guarantee and high-frequency jet ventilation are being increasingly used, particularly in the most immature infants. While evidence remains heterogeneous, there is growing support for their role in carefully selected populations. In the smallest of infants, a first intention approach using endotracheal tubes as small as 2.0 mm is possible and being done to use as gentle an approach to ventilation despite the small size of these infants.[4]
2. Delayed extubation and “Gentle” Respiratory Care
One center with remarkable results in those born at 22-23 weeks by adopting an approach of using gentle ventilation with low pressure on high frequency jet ventilation. These infants are maintained on this strategy for weeks before attempting to extubate. The focus is kept on nutritional support and allowing these infants to establish the necessary muscle, bony support and drive to be successful once extubated and minimizing the trauma to their delicate pulmonary tissue.[5]
3. Caffeine Therapy
Don’t underestimate the importance of this common medication! Early administration (within the first three days of life) reduces BPD, retinopathy of prematurity, and late-onset sepsis, while facilitating earlier extubation.[6]
There is increasing interest in higher dosing strategies, though the balance between efficacy and safety remains under investigation.
4. Surfactant Delivery: The Rise of LISA
Less Invasive Surfactant Administration (LISA) represents one of the most significant practice changes in recent years. By allowing surfactant delivery while maintaining spontaneous breathing, LISA reduces the need for mechanical ventilation and is associated with lower rates of death or BPD in infants <27 weeks.[7]
The Power of Bundled Care
Perhaps the most important insight is that no single intervention is sufficient.
The concept of an integrated care bundle combining early noninvasive support, appropriate surfactant use, early caffeine, targeted oxygen strategies, and selective corticosteroid use is gaining traction.
Standardization through protocols and quality improvement initiatives appears critical. As noted in recent work, “only a multipronged preventive approach has the potential to achieve meaningful reduction in BPD burden.” [8]
Emerging Therapies: Hope or Hype?
Looking forward, several promising therapies are under investigation:
- Mesenchymal stromal cells (MSCs): Strong preclinical data suggests anti-inflammatory and regenerative effects, though early clinical trials have not yet demonstrated clear benefit.[9]
- Anakinra (IL-1 receptor antagonist): Targeting inflammation directly, this approach reflects our evolving understanding of BPD as an inflammatory disease.[10]
- IGF-1/IGFBP-3 therapy: Early trials suggest potential reductions in severe BPD, though concerns about increased mortality highlight the complexity of translating biologic therapies into clinical practice.[11]
So, Does Faith Matter Most?
Faith is the starting point. It takes many care providers to care for one tiny baby. When everyone believes that they can accomplish great things, outcomes are likely to improve. It influences how critically we pay attention to detail, how closely we respond to changes in clinical signs and helps inspire those on the team to do their very best in the face of adversity.
Moreover, it influences how we counsel families, how we allocate resources, and how we define acceptable risk.
But faith alone is no longer sufficient to explain outcomes.
What distinguishes high-performing centres today is not just belief, but execution in the following four domains:
- Consistent application of evidence-based practices
- Rigorous quality improvement
- Attention to detail in respiratory and hemodynamic management
- A commitment to minimizing variability
In other words, faith matters most when paired with discipline. Faith still opens the door but what we do after walking through it is what truly determines outcome.

Dr. Michael Narvey
Neonatologist
University of Manitoba
References
[3] Canadian Neonatal Follow-Up Network. 2023–2024 annual report [Internet]. 2024 [cited 2026 Apr 12]. Available from: https://canadianneonatalfollowup.ca/annual-report/
[4] Berger JN, Elgin TG, Dagle JM, Klein JM, Colaizy TT. Survival and short-term respiratory outcomes of <750 g infants initially intubated with 2.0 mm vs. 2.5 mm endotracheal tubes. J Perinatol. 2022 Feb;42(2):202-208
[11] Ley D, Hallberg B, Hansen-Pupp I, Dani C, Ramenghi LA, Marlow N, Beardsall K, Bhatti F, Dunger D, Higginson JD, Mahaveer A, Mezu-Ndubuisi OJ, Reynolds P, Giannantonio C, van Weissenbruch M, Barton N, Tocoian A, Hamdani M, Jochim E, Mangili A, Chung JK, Turner MA, Smith LEH, Hellström A; study team. rhIGF-1/rhIGFBP-3 in Preterm Infants: A Phase 2 Randomized Controlled Trial. J Pediatr. 2019 Mar;206:56-65.e8